
Page 816 - TNFlipTest
P. 816
NS18 Neurosurgery
Hemicraniectomy in Older Patients with Extensive Middle-Cerebral-Artery Stroke
NEJM 2014;370:1091-1100
Purpose: To determine if early decompressive hemicraniectomy reduces mortality among patients >60 yr.
Study: 112 patients >60 yr (median age 70
yr) with malignant MCA infarction randomly assigned to conservative ICU treatment versus hemicraniectomy. Endpoint was survival without severe disability (modified Rankin scale score 0-4). Results: The proportion of patients who survived without severe disability was 38% in the hemicraniectomy group and 18% in the control group (OR 2.91, 95% CI 1.06-7.49). Modified Rankin scale scores in hemicraniectomy versus control group in terms of percentages of patients: 0-2 (0%, 0%), 3 or moderate disability (7%, 3%),
Cerebrovascular Disease Toronto Notes 2019 Cerebrovascular Disease
Ischemic Cerebral Infarction (80%)
• embolic,thrombosisofintracerebralarteries,vasculitis,hypercoagulability,etc.(seeNeurology,N48) Intracranial Hemorrhage (20%)
• SAH,spontaneousICH,IVH
3 4
6
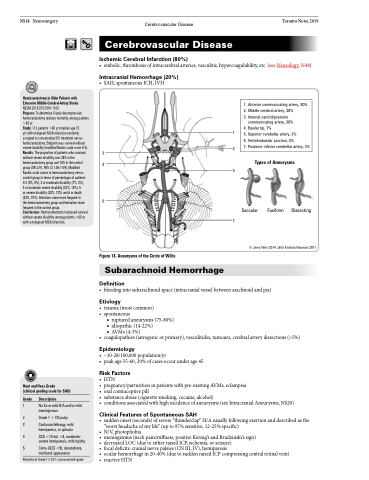
Figure 18. Aneurysms of the Circle of Willis
1 2
5
7
Types of Aneurysms
1. Anterior communicating artery, 30%
2. Middle cerebral artery, 20%
3. Internal carotid/posterior communicating artery, 30%
4. Basilar tip, 7%
5. Superior cerebellar artery, 3%
6. Vertebrobasilar junction, 2%
7. Posterior inferior cerebellar artery, 3%
4 or moderate severe disability (32%, 15%), 5 or severe disability (28%, 13%) and 6 or death (33%, 70%). Infections were more frequent in the hemicraniectomy group and herniation more frequent in the control group.
Conclusions: Hemicraniectomy increased survival without severe disability among patients >60 yr with a malignant MCA infarction.
Saccular
Fusiform
Dissecting
© Jerry Won 2014, after Kristina Neuman 2011
Subarachnoid Hemorrhage
Definition
Hunt and Hess Grade
(clinical grading scale for SAH)
Grade Description
1 No Sx or mild H/A and/or mild meningismus
2 Grade 1 + CN palsy
3 Confusion/lethargy, mild hemiparesis, or aphasia
4 GCS <15 but >8, moderate- severe hemiparesis, mild rigidity
5 Coma (GCS <9), decerebrate, moribund appearance
Mortality of Grade 1-2 20%, increased with grade
• bleedingintosubarachnoidspace(intracranialvesselbetweenarachnoidandpia)
Etiology
• trauma(mostcommon) • spontaneous
■ ruptured aneurysms (75-80%) ■ idiopathic (14-22%)
■ AVMs (4-5%)
• coagulopathies(iatrogenicorprimary),vasculitides,tumours,cerebralarterydissections(<5%)
Epidemiology
• ~10-28/100,000population/yr
• peakage55-60,20%ofcasesoccurunderage45
Risk Factors
• HTN
• pregnancy/parturition in patients with pre-existing AVMs, eclampsia
• oral contraceptive pill
• substanceabuse(cigarettesmoking,cocaine,alcohol)
• conditionsassociatedwithhighincidenceofaneurysms(seeIntracranialAneurysms,NS20)
Clinical Features of Spontaneous SAH
• suddenonset(seconds)ofsevere“thunderclap”H/Ausuallyfollowingexertionanddescribedasthe “worst headache of my life” (up to 97% sensitive, 12-25% specific)
• N/V, photophobia
• meningismus(neckpain/stiffness,positiveKernig’sandBrudzinski’ssign)
• decreasedLOC(duetoeitherraisedICP,ischemia,orseizure)
• focal deficits: cranial nerve palsies (CN III, IV), hemiparesis
• ocularhemorrhagein20-40%(duetosuddenraisedICPcompressingcentralretinalvein) • reactive HTN
