
Page 896 - TNFlipTest
P. 896
OP6 Ophthalmology
The Ocular Examination Toronto Notes 2019
• legalblindnessisBCVAthatis≤20/200inbesteye
• minimumvisualrequirementstooperateanon-commercialautomobileinOntarioare:20/50BCVA
with both eyes open and examined together, 120° continuous horizontal visual field, and 15° continuous visual field above and below fixation
Visual Acuity – Near
• usepocketvisionchart(RosenbaumPocketVisionScreener)
• recordJaeger(J)orPointnumberandtestingdistance(usually30cm)e.g.J2@30cm
• conversiontodistancevisualacuitypossible(e.g.immobilepatient,nodistancechartavailable)
Visual Acuity for Infants, Children, Non-English Speakers, and Dysphasics
• newborns
■ VA cannot be tested conventionally
• 3mo-3yr:canonlyassessvisualfunction,notacuity
■ test each eye for fixation symmetry using an interesting object
■ normal function noted as “CSM” = central, steady, and maintained
• 3yruntilalphabetknown
■ pictures or letter cards/charts such as HOTV or Sheridan-Gardner test (children point to optotypes
on a matching card) ■ tumbling “E” chart
Colour Vision
• testwithIshiharapseudoisochromaticplates
• recordnumberofcorrectlyidentifiedplatespresentedtoeacheye,specifyincorrectplates • importantfortestingopticnervefunction(e.g.opticneuritis,chloroquineuse,thyroid
ophthalmopathy)
• note:red-greencolourblindnessissex-linkedandoccursin7-10%ofmales
VISUAL FIELDS
• test “visual fields by confrontation” (4 quadrants, each eye tested separately) for estimation of visual field loss
• accurate, quantifiable assessment with automated visual field testing (Humphrey or Goldmann) or Tangent Screen
• use Amsler grid (each eye tested separately) to check for central or paracentral scotomas (blindspots) in patients with AMD
PUPILS
• usereducedroomilluminationwithpatientfocusingondistant,fixedobjecttopreventnearreflex
• examinepupilsforshape,size,symmetry,andreactivitytolight(bothdirectandconsensualresponse) • testforRAPDwithswingingflashlighttest,checkbyreverseRAPDifonepupilnon-reactive
• testpupillaryconstrictionportionofnearreflexbybringingobjectclosetopatient’snose
• “normal”pupiltestingoftennotedasPERRLA(pupilsequal,round,reactivetolightand
accommodation)
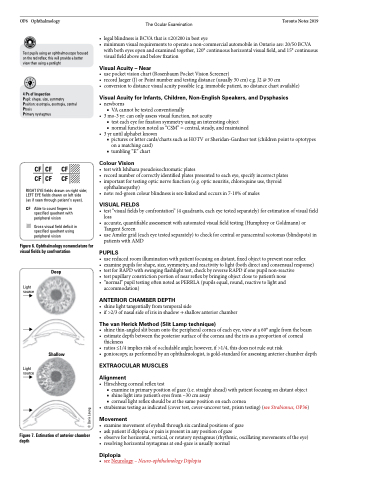
ANTERIOR CHAMBER DEPTH
• shinelighttangentiallyfromtemporalside
• if>2/3ofnasalsideofirisinshadow→shallowanteriorchamber
The van Herick Method (Slit Lamp technique)
• shinethin-angledslitbeamontotheperipheralcorneaofeacheye,viewata60°anglefromthebeam • estimatedepthbetweentheposteriorsurfaceofthecorneaandtheirisasaproportionofcorneal
thickness
• ratios≤1/4impliesriskofoccludableangle;however,if>1/4,thisdoesnotruleoutrisk
• gonioscopy, as performed by an ophthalmologist, is gold-standard for assessing anterior chamber depth
EXTRAOCULAR MUSCLES
Alignment
• Hirschbergcornealreflextest
■ examine in primary position of gaze (i.e. straight ahead) with patient focusing on distant object ■ shine light into patient’s eyes from ~30 cm away
■ corneal light reflex should be at the same position on each cornea
• strabismustestingasindicated(covertest,cover-uncovertest,prismtesting)(seeStrabismus,OP36)
Movement
• examinemovementofeyeballthroughsixcardinalpositionsofgaze
• askpatientifdiplopiaorpainispresentinanypositionofgaze
• observeforhorizontal,vertical,orrotatorynystagmus(rhythmic,oscillatingmovementsoftheeye) • resolvinghorizontalnystagmusatend-gazeisusuallynormal
Diplopia
• seeNeurology–Neuro-ophthalmologyDiplopia
Test pupils using an ophthalmoscope focused on the red reflex; this will provide a better view than using a penlight
4 Ps of Inspection
Pupil: shape, size, symmetry Position: esotropia, exotropia, central Ptosis
Primary nystagmus
CFCF CF
CFCF CF
RIGHT EYE fields drawn on right side; LEFT EYE fields drawn on left side (as if seen through patient’s eyes).
CF Able to count fingers in specified quadrant with peripheral vision
Gross visual field deficit in specified quadrant using peripheral vision
Figure 6. Ophthalmology nomenclature for visual fields by confrontation
Light source
Deep
Light source
Shallow
Figure 7. Estimation of anterior chamber depth
© Doris Leung
